COPY of Patient Care Dorel McAlister DOB 01/02/ 1939
Daily Assessment Record
| Legend: | X= Yes | Date:__________________________ | |||||||||
| System | Normal Criteria | Form | Notes | ||||||||
| Safety: | QPA ☐ | Bedside Safety ☐ | Falls Risk Assessment ☐ | 15 min checks ☐ | |||||||
| Neurological/ Cognition: | Alert & orientated x 3, speech clear and understandable, memory intact, active ROM, sensation intact, no paresthesia ☐ | Delirium Screening ☐ Neuro Vitals ☐ | |||||||||
| Cardiovascular: | Regular apical/peripheral pulse, no chest pain, peripheral pulses palpable, no calf redness, extremities pink and warm ☐ | Telemetry Monitoring ☐ Vascular Form ☐ | |||||||||
| Respiratory: | Resting respirations quiet & regular, symmetrical chest wall movement, pink nail beds and mucous membranes, air entry clear to bases on L&R lobe ☐ | Chest ☐ Tube ☐ Suction ☐ Trach ☐ | |||||||||
| Gastrointestinal | Abdomen soft and non distended, tolerates without nausea, no difficulty swallowing, bowel pattern normal for pt, bowel sounds present ☐ | Last BM ____________ Parenteral Nutrition ☐ Enteral Nutrition ☐ Ostomy ☐ Tube ___________________ | |||||||||
| Genitourinary: | Urinates without pain, voiding pattern is usual, urine clear, yellow ☐ | Urostomy ☐ Foley ☐ | |||||||||
| Gynecology/Urology | Skin intact ☐, no lesions or discharge ☐, no itch or odor ☐ | STI Screening ☐ LMP ____________ | |||||||||
| Musculoskeletal: | Steady gait, no fractures/sprains/strains ☐ | Total Care ☐ 1Person Assist ☐ 2Person Assist ☐ | |||||||||
| Psychosocial: | Interacts and communicates in an appropriate manner with others, demonstrates effective coping skills ☐ | MSE ☐ | |||||||||
| Integumentary: | Color normal, warm, dry and intact, moist mucus membranes ☐ | Braden ☐ Wound Care ☐ Drain_____________ | |||||||||
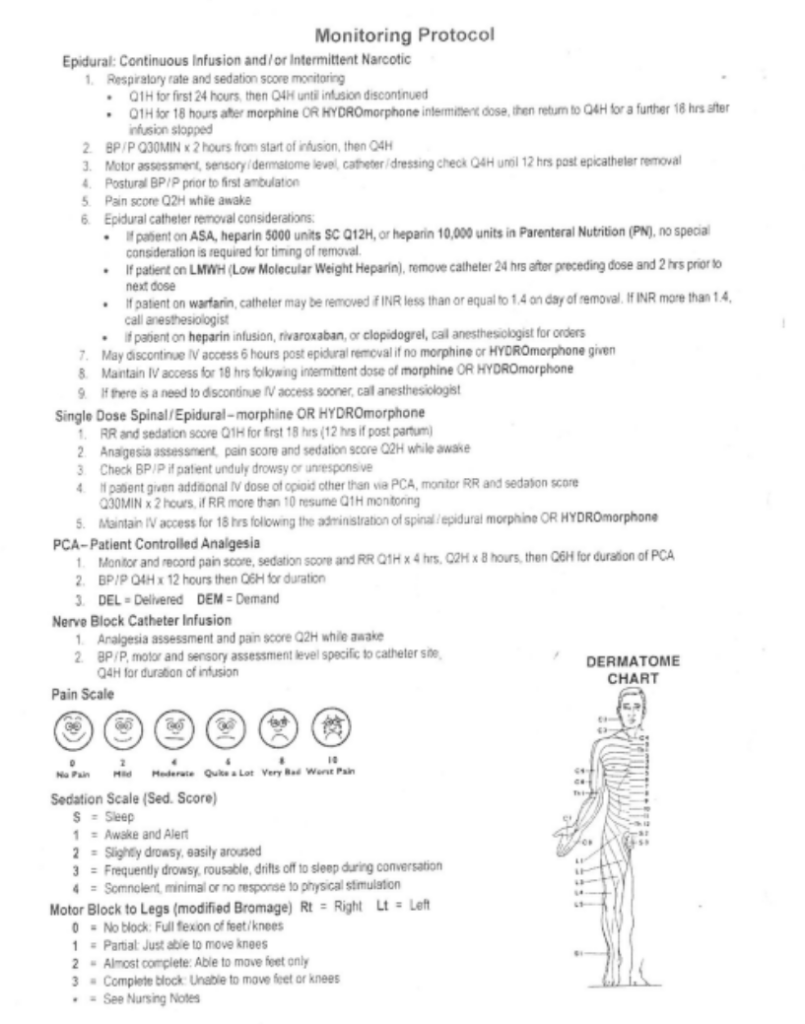
| Pain: | Denies pain ☐ | Pain assessment ☐ | |||||||||
| Other: | |||||||||||
| IV: | Free inflammation, patent, no pain, dressing intact, flushes well ☐ | Type_______ Gauge_______ Location_________ Lumen #____________ | |||||||||
| Date | Nurses Notes (Data/Action/Response/Notes) | Provider | |||||||||
Vital Signs
| DAY | yesterday @ 1930 – today @ 0730 (night shift) | |||||||
| TIME | 2200 | 0600 | ||||||
| TEMPERATURE | 36.2 | 36.9 | ||||||
| PULSE | 84 | 74 | ||||||
| RESPIRATION | 12 | 14 | ||||||
| BLOOD PRESSURE | 100 | 118 | ||||||
| 64 | 64 | |||||||
| O2 SAT | 88% 2L | 88% 2L | ||||||
| Initials | SL | SL | ||||||
| DAY | yesterday 0730-1930 (day shift) | |||||||
| TIME | 0800 | 1200 | 1800 | |||||
| TEMPERATURE | 37.5 | 37.0 | 36.7 | |||||
| PULSE | 82 | 81 | 76 | |||||
| RESPIRATION | 16 | 16 | 14 | |||||
| BLOOD PRESSURE | 135 | 129 | 118 | |||||
| 78 | 79 | 75 | ||||||
| O2 SAT | 95% 3L | 94% 3L | 90% 2L | |||||
| Initials | RA | RA | RA | |||||
| DAY | 2 days ago (admission to nursing unit from PAR 1930-0730) night shift | |||||||
| TIME | 1930 | 2030 | 2130 | 2300 | 0200 | 0600 | ||
| TEMPERATURE | ||||||||
| PULSE | ||||||||
| RESPIRATION | ||||||||
| BLOOD PRESSURE | ||||||||
| O2 SAT | ||||||||
| Weight | ||||||||
| Initials | ||||||||
In/Out Record
| INTAKE | DATE | 24 Hr Total | ||||||
| SHIFT: | Days | Nights | ||||||
| TIME: | ||||||||
| ORAL | ||||||||
| IV | ||||||||
| TUBE FEED | ||||||||
| BLOOD | ||||||||
| TPN | ||||||||
| LIPIDS | ||||||||
| Other | ||||||||
| TOTAL | ||||||||
| OUTPUT | DATE | |||||||
| TIME: | ||||||||
| VOID | ||||||||
| FOLEY | ||||||||
| EMESIS | ||||||||
| Other: | ||||||||
| STOOL | ||||||||
| TOTAL | ||||||||
| 24 hr Balance | ||||||||
SBAR Report
Blood Glucose Record
| Breakfast | Lunch | Dinner | HS | ||
| Date: | |||||
| Time: | |||||
| Reading: | |||||
| Comments: | |||||
| Date: | |||||
| Time: | |||||
| Reading: | |||||
| Comments: | |||||