Patient Care Dorel McAllister DOB 01/02/ 1939
Daily Assessment Record
| Legend: | X= Yes | Date: yesterday | |||||||||
| System | Normal Criteria | Form | Notes | ||||||||
| Safety: | QPA x | Bedside Safety x | Falls Risk Assessment x | minimum 60 minute checks x | |||||||
| Neurological/ Cognition: | Alert & orientated x 3, speech clear and understandable, memory intact, active ROM, sensation intact, no paresthesia x see notes | pain management flowsheet x | |||||||||
| Cardiovascular: | Regular apical/peripheral pulse, no chest pain, peripheral pulses palpable, no calf redness, extremities pink and warm, no edema x | n/a | |||||||||
| Respiratory: | Resting respirations quiet & regular, symmetrical chest wall movement, pink nail beds and mucous membranes, air entry clear to bases on L&R lobe ☐ -see notes | n/a | |||||||||
| Gastrointestinal | Abdomen soft and non distended, tolerates diet without nausea, no difficulty swallowing, bowel pattern normal for pt, bowel sounds present ☐ – see notes | Last BM preop | |||||||||
| Genitourinary: | Urinates without pain, voiding pattern is usual, urine clear, yellow ☐ – see note | Foley x | |||||||||
| Gynecology/Urology | Perineal skin intact x, no lesions or discharge x no itch or odor x | n/a | |||||||||
| Musculoskeletal: | Steady gait, no fractures/sprains/strains ☐ – see notes | 1Person Assist x | |||||||||
| Psychosocial: | Interacts and communicates in an appropriate manner with others, demonstrates effective coping skills x | MSE x | |||||||||
| Integumentary: | Color normal, warm, dry and intact, moist mucus membranes ☐ see notes | Braden x Wound Care ☐ Drain – JP abdomen | |||||||||
| Pain: | Denies pain ☐ – see notes | pain management flow sheet x | |||||||||
| Other: | —- | —- | |||||||||
| IV: | Free of inflammation, patent, no pain, dressing intact, flushes well x | Type: PVAD short Gauge: 22 Location: right forearm Lumen #: 1 | |||||||||
| Date | Nurses Notes (Data/Action/Response/Notes) | Provider | |||||||||
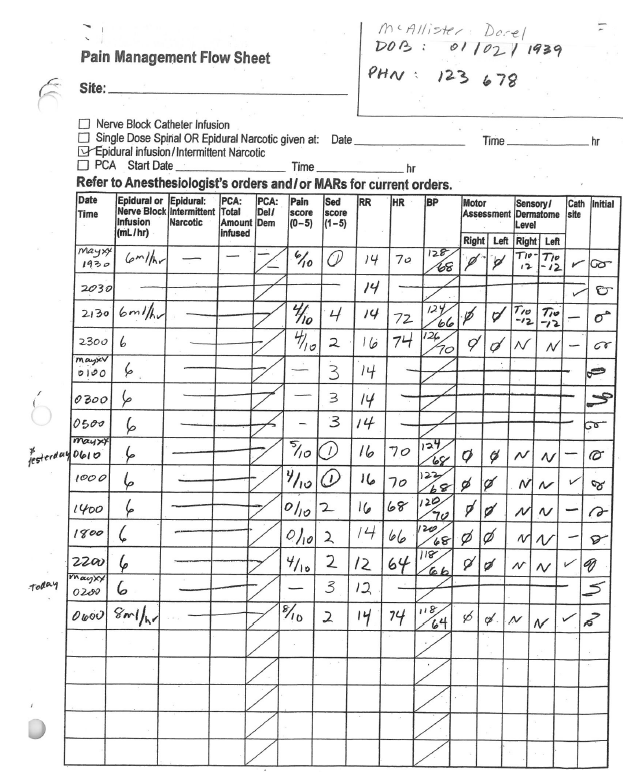
| 2 days prior @1930 | Admitted from PAR. Alert & oriented x3. Epidural infusion bupivacaine / fentanyl @ 6cc/hr. See flowsheet. Abdominal pain 6/10. Sharp. Abdominal splint provided. Sensory block present T10-T12 bilaterally. No evidence of motor block. Decreased air entry bilateral bases. DB&C instructed & encouraged hourly while awake. O2@ 5L / NP. SpO2 93%. RR 14. Abdomen soft, flat. no bowel sounds. denies flatus. Foley insitu. Clear amber urine. Abdominal dressing dry & intact. JP drain emerging from dressing. Scant sanguineous drainage present. All limbs warm. Brisk cap refill. 128/68 HR 70 regular ———————————————————————————————————– | DG RN | |||||||||
| yesterday @ 0740 | Dr. James aware of abnormal bloodwork. No orders received. No evidence of active bleeding. | RA RN | |||||||||
| last night @ 2200 | Epidural infusion bupivacaine / fentanyl @ 6 mL/hr. Describes abdominal pain4/10. Diminished air entry bilateral bases. Reports DB&C hourly while awake. Patient able to demonstrate effective use of incentive inspirometer. SPO2 92% 4L/ nasal prongs. RR 12. Foley insitu. Clear amber urine. 1person assist to bathroom. Gait strong bilaterally. Requires assurance. Declines offer of walker. Abdominal dressing scant shadowing. JP scant sanguineous. Tolerating clear fluids. Denies nausea. | SL RN | |||||||||
| today 0600 | Weight 105 kg. Increase of 5 kg since admission. Abdominal pain sharp, central lower abdomen. 8/10. Non radiating. Epidural bupivacaine fentanyl increased 8cc/ hr. | SL RN | |||||||||
Vital Signs
| DAY | yesterday @ 1930 – today @ 0730 (night shift) | |||||||
| TIME | 2200 | 0200 | 0600 | |||||
| TEMPERATURE | 36.2 | —- | 36.9 | |||||
| PULSE | 64 | —- | 74 | |||||
| RESPIRATION | 12 | 12 | 14 | |||||
| BLOOD PRESSURE | 118 | —- | 118 | |||||
| 66 | —- | 64 | ||||||
| SpO2 / supplemental oxygen | 92% 4L | —- | 92%5L | |||||
| Weight Initials | —- SL | —- SL | 105 kg SL | |||||
| DAY | yesterday 0730-1930 (day shift) | |||||||
| TIME | 1000 | 1400 | 1800 | |||||
| TEMPERATURE | 37.5 | 37.5 | 36.0 | |||||
| PULSE | 70 | 70 | 68 | |||||
| RESPIRATION | 16 | 16 | 14 | |||||
| BLOOD PRESSURE | 122 | 120 | 120 | |||||
| 68 | 70 | 68 | ||||||
| SpO2 / supplemental oxygen | 95% 3L | 95% 3L | 92% 2L | |||||
| Weight Initials | 101kg RA | —- RA | —- RA | |||||
| DAY | 2 days ago – admission to nursing unit from PAR 1930-0730 (night shift) | |||||||
| TIME | 1930 | 2030 | 2130 | 2300 | 0200 | 0600 | ||
| TEMPERATURE | 36.5 | —- | —- | 37.0 | —- | 36.5 | ||
| PULSE | 70 | —- | 72 | 74 | —- | 70 | ||
| RESPIRATION | 14 | 14 | 14 | 16 | 14 | 16 | ||
| BLOOD PRESSURE | 128 | —- | 124 | 126 | —- | 124 | ||
| 68 | —- | 66 | 70 | —- | 68 | |||
| SpO2 / supplemental O2 | 93% / 5L | —- | —- | 93% / 5L | —- | —- | ||
| Weight | 100kg | —- | —- | —- | —- | —- | ||
| Initials | DG | DG | DG | DG | DG | DG | ||
Pain Management Flowsheet
In/Out Record
| INTAKE | DATE | yesterday | 24 Hr Total | |||||
| SHIFT: | Day shift 0730-1930 *yesterday | night shift 1930-0730 *last night | ||||||
| TIME: | 1300 | 1500 | 1930 | 0100 | 0700 | |||
| ORAL | sips | 100 | 100 | 100 | 125 | |||
| IV | 360 | 120 | 240 | 330 | 360 | |||
| TUBE FEED | —- | —- | ||||||
| BLOOD | —- | —- | ||||||
| TPN | —- | —- | ||||||
| LIPIDS | —- | —- | ||||||
| Other | —- | —- | ||||||
| TOTAL | 360 | 220 | 340 | 430 | 485 | 1835 | ||
| OUTPUT | DATE | Day shift 0730-1930 *yesterday | ||||||
| TIME: | 1300 | 1500 | 1930 | 0100 | 0700 | |||
| VOID | —- | —- | —- | —- | —- | |||
| FOLEY | 165 | 75 | 130 | 165 | 180 | |||
| EMESIS | 0 | 0 | 0 | 0 | 0 | |||
| Other: JP | scant | 0 | 0 | 0 | 0 | |||
| STOOL | 0 | 0 | 0 | 0 | 0 | |||
| TOTAL | 165 | 75 | 130 | 165 | 180 | 715 | ||
| 24 hr Balance | Note: Today @ 0730: + 645 mL carried from previous shift PLUS 1120 mL today = +1765mL SL RN | +1120 | ||||||
| INTAKE | DATE | 2 days prior | 24 Hr Total | ||||||
| SHIFT: | Days | Nights 1930 – 0730 * admitted from PAR@1930 | |||||||
| TIME: | —- | —- | —- | —- | from OR/ PAR | 0130 | 0700 | ||
| ORAL | —- | —- | —- | NPO | sips | sips | |||
| IV | —- | —- | —- | 300mL | 360 | 360 | |||
| TUBE FEED | —- | —- | —- | —- | —- | —- | |||
| BLOOD | —- | —- | —- | —- | —- | —- | |||
| TPN | —- | —- | —- | —- | —- | —- | |||
| LIPIDS | —- | —- | —- | —- | —- | —- | |||
| Other | —- | —- | —- | —- | —- | —- | |||
| TOTAL | —- | —- | —- | 300 | 360 | 360 | 1020 | ||
| OUTPUT | DATE | Days | Nights 1930 – 0730 *admitted from PAR@1930 | ||||||
| TIME: | OR/ PAR | 0130 | 0730 | ||||||
| VOID | —- | —- | —- | —- | —- | —- | —- | ||
| FOLEY | —- | —- | —- | —- | 30 | 180 | 165 | ||
| EMESIS | —- | —- | —- | —- | 0 | 0 | 0 | ||
| Other: JP | —- | —- | —- | —- | scant | 0 | 0 | ||
| STOOL | —- | —- | —- | —- | —- | —- | —- | —- | |
| TOTAL | —- | —- | —- | —- | 30 | 180 | 165 | 375 | |
| 24 hr Balance | +645 | ||||||||