Patient Care – Mel LaFleur
Daily Assessment Record
| Legend: | ☒ = Yes | Date: Post operative 12 hrs | |||||||||
| System | Data | Form | Notes | ||||||||
| Safety: | QPA ☒ | Bedside Safety ☒ | Falls Risk Assessment ☒ | 15 min checks ☒ | |||||||
| Neurological/ Cognition: | Alert & orientated x 2, not orientated to time, speech clear and understandable, sensation intact throughout body, no paresthesia. | Delirium Screening ☒ Neuro Vitals ☐ | |||||||||
| Cardiovascular: | Regular apical/peripheral pulse, no chest pain, peripheral pulses palpable, extremities pink and warm, Brisk Capp refill to extremities | Telemetry Monitoring ☐ Vascular Form ☐ | |||||||||
| Respiratory: | Respirations adequate, course crackles to bases with productive cough with thick yellow sputum, symmetrical chest wall movement, pink nail beds and mucous membranes. | Chest ☐ Tube ☐ Suction ☐ Trach ☐ | |||||||||
| Gastrointestinal | Abdomen soft and non distended, mild nausea, no difficulty swallowing, has not had bowel movement since admission, bowel sounds present. | Last BM _Unknown____ Parenteral Nutrition ☐ Enteral Nutrition ☐ Ostomy ☐ Tube ___________________ | |||||||||
| Genitourinary: | Urinates without pain, voiding pattern is usual, urine clear, yellow. | Urostomy ☐ Foley ☒ | |||||||||
| Gynecology/Urology | Skin intact, no lesions or discharge, no itch or odor. | STI Screening ☐ LMP ____________ | |||||||||
| Musculoskeletal: | Remains resting in bed awaiting physiotherapy. Able to mildly dorsi and planter flex right foot. Ice applied for comfort ice applied. Turning frequently in bed. SCDs in place bilaterally. | Total Care ☐ 1Person Assist ☐ 2Person Assist ☒ | |||||||||
| Psychosocial: | Interacts and communicates in an appropriate manner with others, demonstrates effective coping skills. Spoke to daughter on phone earlier today. | MSE ☒ | |||||||||
| Integumentary: | Color normal, skin warm, dry and intact, moist mucus membranes. Dressing to Rt hip intact, scant amount of dime size oozing noted to dressing. Mild warmth around right surgical site. | Braden ☒ Wound Care ☒ Drain_____________ | |||||||||
| Pain: | Pain to right hip 7/10, describes as sharp stabbing and radiating into right foot. | Pain assessment ☒ | |||||||||
| Other: | |||||||||||
| IV: | IV site free inflammation, patent, no pain, dressing intact, flushes well. | Type:______PVAD-S_____ Gauge:____ 20__ Location:___Rt hand_____ Lumen #___ 1________ | |||||||||
| Date Focus | Nurses Notes (Data/Action/Response/Notes) | Provider | |||||||||
Vital Signs
| DAY: Day of admission | ||||||||
| TIME | 1400 | 1800 | 2100 | |||||
| TEMPERATURE | 38.3 | 38 | 37.5 | |||||
| PULSE | 90 | 84 | 88 | |||||
| RESPIRATION | 24 | 22 | 20 | |||||
| BLOOD PRESSURE | 166 | 140 | 140 | |||||
| 88 | 75 | 75 | ||||||
| O2 SAT | 86 | 92 | 94 | |||||
| WEIGHT | 80 kg | |||||||
| Initials | PN | PN | DG | |||||
| DAY: post op q12 hrs | ||||||||
| TIME | 0800 | 1200 | 1700 | 2100 | ||||
| TEMPERATURE | 36.7 | 36.4 | 36.7 | 36.6 | ||||
| PULSE | 86 | 77 | 75 | 72 | ||||
| RESPIRATION | 16 | 18 | 18 | 16 | ||||
| BLOOD PRESSURE | 138 | 141 | 141 | 138 | ||||
| 72 | 72 | 75 | 70 | |||||
| O2 SAT | 93 | 94 | 93 | 94 | ||||
| Weight | ||||||||
| Initials | PN | PN | DG | DG | ||||
| DAY | ||||||||
| TIME | ||||||||
| TEMPERATURE | ||||||||
| PULSE | ||||||||
| RESPIRATION | ||||||||
| BLOOD PRESSURE | ||||||||
| O2 SAT | ||||||||
| Weight | ||||||||
| Initials | ||||||||
SBAR Report
In/Out Record
| INTAKE | DATE | Post op Day 1 | 24 Hr Total | |||||
| SHIFT: Day | Days | Nights | ||||||
| TIME: | 0900 | 1300 | 1800 | 2100 | 0100 | 0600 | ||
| ORAL | 0 | 100 | 400 | 240 | 60 | 325 | 1125 | |
| IV | 75cc/hr= | 1800 | ||||||
| TUBE FEED | ||||||||
| BLOOD | ||||||||
| PN | ||||||||
| LIPIDS | ||||||||
| Other | ||||||||
| TOTAL | 2925 | |||||||
| OUTPUT | SHIFT: Day | |||||||
| TIME: 1900 | ||||||||
| VOID | ||||||||
| FOLEY | 1500 | 800 | 2300 | |||||
| EMESIS | 200 | 200 | ||||||
| Other: | ||||||||
| STOOL | ||||||||
| TOTAL | ||||||||
| 24 hr Balance | +425 | |||||||
Blood Glucose Record
| Breakfast | Lunch | Dinner | HS | ||
| Date: Day of admission | |||||
| Time: | 1730 | 2130 | |||
| Reading: | 11.8 | 13.7 | |||
| Comments: | |||||
| Date: Post op day 1 | |||||
| Time: | 0730 | 1130 | 1730 | 2130 | |
| Reading: | 8.9 | 9.9 | 11.2 | 12.6 | |
| Comments: | |||||
Braden Scale
| DATE/TIME OF ASSESSMENT: | ||||||||
| Sensory perception Ability to respond meaningfully to pressure-related discomfort | 1. Completely limited: Unresponsive (does not moan, flinch, or grasp) to painful stimuli, due to diminished level of consciousness or sedation, OR Limited ability to feel pain over most of body surface | 2. Very limited: Responds only to painful stimuli. Cannot communicate discomfort except by moaning or restlessness, OR Has a sensory impairment which limits the ability to feel pain or discomfort over ½ of body. | 3. Slightly limited: Responds to verbal commands but cannot always communicate discomfort or need to be turned, OR Has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities. | 4. No impairment: Responds to verbal commands. Has no sensory deficit which would limit ability to feel or voice pain or discomfort. | ||||
| Moisture Degree to which skin is exposed to moisture | 1. Constantly moist: Skin is kept moist almost constantly by perspiration, urine, etc. Dampness is detected every time patient is moved or turned. | 2. Moist: Skin is often but not always moist. Linen must be changed at least once a shift. | 3. Occasionally moist: Skin is occasionally moist, requiring an extra linen change approximately once a day. | 4. Rarely moist: Skin is usually dry; linen requires changing only at routine intervals. | ||||
| Activity Degree of physical activity | 1. Bedfast: Confined to bed. | 2. Chairfast: Ability to walk severely limited or non-existent. Cannot bear own weight and/or must be assisted into chair or wheelchair. | 3. Walks occasionally: Walks occasionally during day but for very short distances, with or without assistance. Spends majority of each shift in bed or chair. | 4. Walks frequently: Walks outside the room at least twice a day and inside room at least once every 2 hours during waking hours. | ||||
| Mobility Ability to change and control body position | 1. Completely Immobile: Does not make even slight changes in body or extremity position without assistance. | 2. Very limited: Makes occasional slight changes in body or extremity position but unable to make frequent or significant changes independently. | 3. Slightly limited: Makes frequent though slight changes in body extremity position independently. | 4. No limitations: Makes major and frequent changes in position without assistance. | ||||
| Nutrition Usual food intake pattern | 1. Very poor: Never eats a complete meal. Rarely eats more than ⅓ of any food offered. Eats 2 servings or less of protein (meat or dairy products) per day. Takes fluids poorly. Does not take a liquid dietary supplement, OR Is NPO1 and/or maintained on clear liquids or IV2 for more than 5 days. | 2. Probably Inadequate: Rarely eats a complete meal and generally eats only about ½ of any food offered. Protein intake includes only 3 servings of meat or dairy products per day. Occasionally will take a dietary supplement, OR Receives less than optimum amount of liquid diet or tube feeding. | 3. Adequate: Eats over half of most meals. Eats a total of 4 servings of protein (meat, dairy products) each day. Occasionally will refuse a meal, but will usually take a supplement of offered, OR Is on a tube feeding or TPN3 regimen, which probably meets most of nutritional needs. | 4. Excellent: Eats most of every meal. Never refuses a meal. Usually eats a total of 4 or more servings of meat and dairy products. Occasionally eats between meals. Does not require supplementation. | ||||
| Friction and Shear | 1. Problem: Requires moderate to maximum assistance in moving. Complete lifting without sliding against sheets is impossible. Frequent slides down in bed or chair, requiring frequent repositioning with maximum assistance. Spasticity, contractures, or agitation leads to almost constant friction. | 2. Potential problem: Moves feebly or requires minimum assistance. During a move, skin probably slides to some extent against sheets, chair, restraints, or other devices. Maintains relatively good position in chair or bed most of the time but occasionally slides down. | 3. No apparent problem: Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move. Maintains good position in be or chair at all times. | |||||
| TOTAL SCORE: | ||||||||
| Signature | Initials | |||||||
Falls Risk Assessment
| RISK FACTOR PRESENT | ☐ ☒ | STRATEGIES |
| More than 2 falls in previous 6 months Move in facility in the past month Dates of falls: Safety awareness: Attempts to unsafely TRANSFER or WALK Not following instructions, agitation, restlessness | ☒ Yes ☐ No ☒ Yes ☐ No | Review history of falls from fall reports ☐ Hip protectors ☐ Fall mat in place ☒ Bed in low position for person’s height ☐ Lower rails down ☒ Use of mobility aid within reach with brakes on ☐ Head protectors |
| Orthostatic hypotension, hypertension/vertigo Check difference in Stood Pressure Date: 1 day after admission Lying: _____136/76_________________________________ Sitting:____140/78_________________________________ | ☒ Yes ☐ No __________ | ☐ Educate resident on how to best transfer and change position when appropriate ☐ Refer to Pharmacist, Physician & other members of the interdisciplinary |
| Cognitive alterations: (e.g., delirium, acquired brain injury, dementia, mental health disorders, infection) Mood alteration such as depression, agitation | ☒Yes ☐ No | ☐ Develop Care Plan to support residents routines and preferences ☐ Utilize bed/chair check, movement alarm, resident wandering system, or motion detector |
| Impaired mobility, balance or gait | ☒ Yes ☐ No | Assess for ☒ Proper shoes, non slip socks for night use ☒ Appropriate walking aid, hip protectors ☒ Refer to PT/OT for exercises, seating, etc. |
| Generalized weakness What is the ambulation ability? _immobile____________________________ What is the transfer ability? ____2PA__________________________________ What is the bed mobilty? ____1PA____________________________________ What is the nutrition risk? ________________________________________ | ☒ Yes ☐ No | ☒ Refer to PT/OT ☐ Safe Transfer _____________ Bed Mobility __1PA______________ ☒ Pain ____________________ ☐ Refer to RD (if poor intake and significant weight loss) |
| Visual/Perceptual deficits | ☐ Yes ☒ No | Assess for ☐ Declutter the room ☐ Refer to Optometrist ☐ Provide sufficient lighting in the room/hallway |
| Urinary and bowel elimination – urgency & frequency | ☐ Yes ☒ No | ☐ Review Voiding Record/Bowel Record to establish regular bladder/bowel routine ☐ Ensure the client is able to safely toilet self or have care team follow the routine |
| Medication and substance use: ☒ Antidepressants ☒ Antihypertensive ☐ Alcohol ☐ Benzodiazepine ☒ Anagesics/Opiods ☒ Diabetic medications ☐ Antipsychotics ☐ Poly pharmacy ☐ Sedatives/Hypnotics | ☒ Yes ☐ No | ☐ Ensure Medications are appropriate – dosage and medication form are easily taken ☒ Consult with Pharmacist or Physician ☐ Medication review done |
Mental Status Exam
| Date Time | Mental Status Exam (MSE) | Notes Required |
| General Appearance: Age Hygiene/Grooming Build | ☐ Appears stated age ☐ Appears younger than age ☐ Appears older than age ☐ Clean ☐ Body odor ☐ Tattoos ☐ Dressed appropriately to season ☐ Unkempt ☐ Average ☐ Frail ☐ Obese ☐ Muscular ☐ Petite ☐ Stocky | |
| Behavior: Eye contact Attitude LOC Activity Level Posture | ☐ Poor ☐ Adequate ☐ Good ☐ Intense ☐ Engaging ☐ Disengaged ☐ Cooperative ☐ Guarded ☐ Open ☐ Fearful ☐ Demanding ☐ Defensive ☐ Suspicious ☐ Alert ☐ Confused ☐ Sedated/drowsy ☐ Hyper alert ☐ Fluctuating ☐ Normal ☐ Pacing ☐ Posturing ☐ Apraxia ☐ Wringing hands ☐ Wandering ☐ Relaxed ☐ Rigid ☐ Slumped ☐ Erect | |
| Mood: (reported by client) | ☐ Afraid ☐ Angry ☐ Anxious ☐ Depressed ☐ Energetic ☐ ☐ Frustrated ☐ Happy ☐ Upset ☐ Overwhelmed ☐ Lonely ☐ Worried ☐ Normal | |
| Affect: Stability/Range Congruency | ☐Angry ☐ Depressed ☐ Anxious ☐ Euphoric ☐ Fearful ☐ Irritable ☐ Suspicious ☐ Euthymic ☐ Labile ☐ Blunted ☐ Flat ☐ Full ☐ Range Is Affect congruent with content of speech and circumstances? ☐ Yes ☐ No | |
| Risk: Suicide Risk Prior Suicide Behavior Level of risk to client Safety Plan completed? Homicidal Ideation | Ideation: ☐ Yes ☐ No ☐ Unknown Plan: ☐ Yes ☐ No ☐ Unknown Resources: ☐ Yes ☐ No ☐ Unknown Means: ☐ Yes ☐ No ☐ Unknown Distress/Pain: ☐ Yes ☐ No ☐ Unknown Triggers: Yes No Unknown Lost someone close to suicide: ☐ Yes ☐ No ☐ Unknown ☐ Yes ☐ No ☐ Unknown Details: Has patient made a suicide attempt or engaged in significant intentional self-harm behaviour within the past 24 hours? ☐ Yes ☐ No ☐ Unknown Comments: (observed by clinician) ☐ None ☐ Mild ☐ Moderate ☐ High/Imminent ☐ Yes ☐ No Details ☐ Yes ☐ No ☐ Unknown Details: | |
| Thought Process: | ☐ Disorganized ☐ Normal ☐ Spontaneous ☐ Poverty ☐ Thought Blocking ☐ Vague ☐ Logical ☐ Perseverative | |
| Speech: Amount Rate Pressure Associations Rhythm | ☐ Normal ☐ Mute ☐ Monosyllabic Clarity: ☐ Clear ☐ Incoherent ☐ Slurred ☐ Normal ☐ Controlled ☐ Slowed ☐ Rapid Volume: ☐ Loud ☐ Moderate ☐ Soft ☐ Normal ☐ Low ☐ Pressured ☐ Explosive ☐ Normal ☐ Loose ☐ Flight of ideas ☐ Word Salad ☐ Tangential ☐ Normal ☐ Even ☐ Hesitant ☐ Stuttering | |
| Thought Content: Delusions Unusual content ??? | ☐ Compulsion ☐ Depressive ☐ Risk to self/others ☐ Thoughts about future ☐ Control ☐ Somatic ☐ Mind reading ☐ Persecution ☐ Grandiosity ☐ Thought broadcasting ☐ Obsessions ☐ Phobias ☐ Preoccupations ☐ Ruminations ☐ Congruent to situation | |
| Perceptual Abnormalities: Hallucinations | ☐ Depersonalization ☐ De-realization ☐ Illusions ☐ None observed ☐ Auditory (command) ☐ Auditory (non-command) ☐ Visual ☐ Denies | |
| Cognition: Memory Attention Orientation Concentration | ☐ Intact ☐ Deficits ☐ Good ☐ Mildly distracts ☐ Unable to attend ☐ Person ☐ Place ☐ Time ☐ Good ☐ Fair ☐ Poor | |
| Insight Reasoning/Judgement | ☐ Full ☐ Partial ☐ Limited ☐ Minimal ☐ Absent ☐ Intact ☐ Mild impairment ☐ Moderate impairment ☐ Severe impairment | |
| Notes: |
Wound Care (WIP)
| Wound Type/Etiology (if known) Pressure ☐ Venous ☐ Arterial ☐ Diabetic ☐ Surgical 2°Intent ☐ Skin Tear ☐ Other ☐ | |||
| If Pressure Ulcer, chart stage: Stage 1_________ Stage 2_________ Stage3_________ Stage 4_________ Stage X(unstageable)_________ Stage SDTI (Suspected Deep Tissue Injury)_________ | |||
| MARK LOCATION OF WOUND/ULCER WITH AN ARROW OR AN ”X” | |||
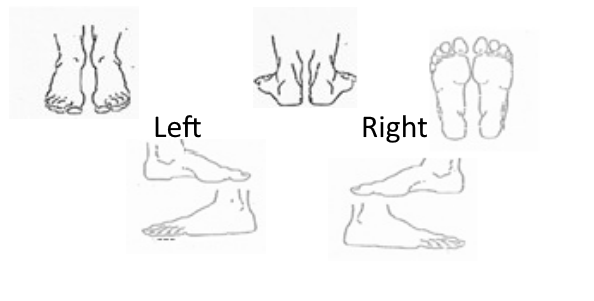 | 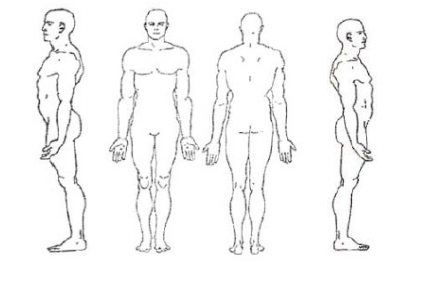 | 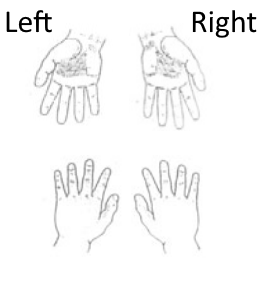 | |
| Legend: X or Blank Space = Not Applicable (as per agency) I * = Assessed/Completed I PN = See Progress Notes | |||
| Wound Location: | Date: | Date: | |
| Time: | Time: | ||
Measurements | Length | ||
| Width | |||
| Depth | |||
| Sinus Tract #1 Depth | |||
| Location (o’clock) | |||
| Sinus Tract #2 Depth | |||
| Location (o’clock) | |||
| Undermining #1 Depth | |||
| Location (o’clock) | |||
| Undermining #2 Depth | |||
| Location (o’clock) | |||
| Wound Bed: Total % must = 100% | % Pink/Red | ||
| % Granulation (red pebbly) | |||
| % Slough | |||
| % Eschar | |||
| % Foreign body (sutures, mesh, hardware) | |||
| % Underlying structures (fascia, tendon, bone) | |||
| % Not visible | |||
| % Other: | |||
| Exudate Amount | None | ||
| Scant/small | |||
| Moderate | |||
| Large/copious | |||
| Exudate Type | Serous | ||
| Sanguineous | |||
| Purulent | |||
| Other: | |||
| Odor | Odour present after cleansing Yes or No | ||
| Wound Edge | Attached (flush w/ wound bed or ”sloping edge”) | ||
| Non-Attached (edge appears as a ”cliff”) | |||
| Rolled (curled under) | |||
| Epithelialization | |||
| Peri-wound Skin | Intact | ||
| Erythema (reddened) in cm | |||
| Indurated (firmness around wound) in cm | |||
| Macerated (white, waterlogged) | |||
| Excoriated/Denuded (superficial loss of tissue) | |||
| Callused | |||
| Fragile | |||
| Other: | |||
| Wound Pain (10 = worst) | Scored from 10 point analogue Pain Scale See Pain Assessment for details | ||
| Treatment | If packing used, indicate # of packing pieces out/in | Out= _____ In=_____ | Out= _____ In=_____ |
| Treatment Plan | |||
| Date Initiated: | |||
| Plan: | |||
| Date D/C: | |||
| Date Initiated: | |||
| Plan: | |||
